Science
in Christian Perspective
Science
in Christian PerspectiveScience
in Christian Perspective
From: JASA 35 (March 1983): 25-32.
Community mental health is concerned with the promotion of mental health and the prevention of mental illness where emphasis is laid on practice within the community. Its target of intervention focuses upon a defined population or community as opposed to individual patients. This approach is based upon the importance of systems of services provided by a community which opts for the continuity of care of services within the community and the provision of indirect services such as consultation and education.
The present discussion is concerned with the affirmation of the community mental health paradigm by Christian theology. Both theology and community mental health are seen as being derived from a single world view which is exemplified by Thomas Oden's "covenant ontology" and Gary Collins' premise of God as the source of all truth. From this, the basic assumptions of positive mental health, prevention of mental disorders, and the social-environmental influences in the community mental health system are supported by theology. A topical discussion of non-professionals, paraprofessionals, and therapeutic considerations is undertaken with implications for future direction in this field.
Community mental health and community psychology are intimately related disciplines that offer the field of psychology an entirely new approach to the health and welfare of individuals in modern society. The two disciplines remain distinct basically in terms of their target of intervention (Iscoe and Spielberger, 1970). Community mental health focuses primarily upon innovative interventions aimed at the individual whereas community psychology is concerned with interventions geared toward the social systems that impinge upon the individual. The two fields represent a "third mental health movement" (Hobbs, 1964) that proclaims a radically new approach to human functioning and as a result its impact upon the professional psychological community is widespread.
Does this third force in psychology represent a legitimate and viable alternative to traditional modes of service delivery, or is it another passing fad ... as Dunham (1965) has put it, another "therapeutic bandwagon?" The answer formulates the central theme for this discussion: When viewed from a theological perspective, the fields of community mental health and community psychology do represent disciplines that possess great potential. Theology may speak directly to these fields by sanctioning their existence and growth as they apply themselves to the treatment of the human condition. This discussion focuses upon the area of community mental health, although it overlaps with community psychology, community psychiatry, and social psychiatry.
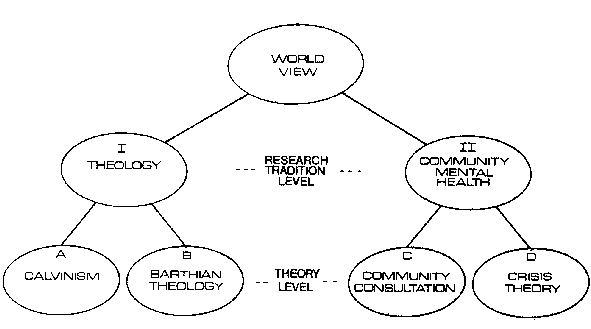
A Model of IntegrationFor one to postulate an integration between theology and community mental health, an examination of each discipline's ontology is warranted. Laudan (1977) provides a model within which this integration may be conceptualized and thereby provides a basis from which a common ontology may be elucidated. Laudan's model is illustrated in Figure I in which there are three levels of inquiry: the world view, the research tradition level, and the theory level.
Research tradition level. In his model, the research tradition is defined as
A set of general assumptions about the entities and processes in a domain of study, and about the appropriate methods to be used for investigating the problems and constructing the theories in that domain. (p.81)
Thus, each research tradition embodies an ontology for the entities within the research tradition and also provides methods of inquiry into those entities. In essence, as Laudan has stated, "a research tradition is thus a set of ontological and methodological 'do's' and 'don'ts"' (p.80).
Theory level. At a lower level stemming from the research
traditions are the theories. Theories speak about specific and
testable laws about nature. Thus, the theory is a necessary and
vital link between empirical observations and the ontologies
of the research tradition.
The present discussion focuses on Laudan's model in the
following manner. Research tradition I represents the discipline of theology. To illustrate, particular theories that may
generate from this research tradition are: Theory A-Calvinism; Theory B-Barthian Theology. Research tradition 11
represents the field of community mental health. Some
theories that grow out of this research tradition are: Theory
C-Community Consultation; Theory D-Crisis Theory.
World view. At the highest level of inquiry in Laudan's model is the world view that entails particular research traditions. It is at this level that an ontology is defined from which the research traditions of theology and community mental health are commonly derived. If these two disciplines have a common ontology, then they share common elements. Laudan has stated that certain elements are more central to the research tradition and in turn become characteristic of that research tradition. The research traditions of theology and community mental health share common core elements derived from a common ontology. Although both research traditions embody common core elements, there are elements (e.g. methodologies) that are unique to each discipline. However, the commonality of the elements characteristic to each research tradition provides a foundation for the affirmation of community mental health by theology. The next step, then, is to elucidate the common ontology (i.e. world view) that provides the basis for relating theology and community mental health.
Covenant Ontology as a World View'Ontology' means the study of being, or inquiry into the nature and modes of being. 'Covenant' means the relation that God has chosen and established with the world and man, as seen prototypically in the history of the people of Israel and therefore representatively with all creation, embracing all being, the essential terms of which are: 'They shall be my people, and I will be their God' (jer.32:38). Covenant ontology is therefore a study of being which sees being as existing in covenant and the covenant of God as the center and circumference of being. (p.78)
The world view is that all being is in covenant relationship with God who is also the core and parameter of creation. It follows that any derivative of being must also be rooted in the covenant ontology. Theology is rooted in a covenant ontology in the same way that community mental health is rooted in a covenant ontology ... they derive from the same source. Herein lies the basis for the affirmation of community mental health by theology. Each discipline embodies God's unconditional love for his people. Indeed, the covenant of grace was given to all.
I will establish my covenant as an everlasting covenant between me and you and your descendants after you for the generations to come, to be your God and the God of your descendants after you. The whole land of Canaan, where you are now an alien, I will give as an everlasting possession to you and your descendants after you; and I will be their God. (Genesis 17:7-8)
The characteristic that distinguishes, for example, Christian fellowship (i.e. the dynamics of a fellowship community) and the community mental health notion of "community functions" (Klein, 1968) is that the former explicitly proclaims God as the source of its existence and functioning whereas the latter implicitly embodies God's design. There is an implicit function working within the community mental health domain that can be made explicit in the theological domain. This is Oden's assumption of the covenant ontology, both implicitly and explicitly proclaimed. The separation of the two research traditions stems from the idea that community mental health is not conscious of its ontological presupposition whereas theology consciously proclaims it. This is not to say that community mental health was born out of the ontological presupposition of God's covenant of grace (though it embraces grace implicitly). In fact, community mental health came about because of a number of dissatisfactions and deficits in traditional mental health service delivery systems (Korchin, 1976). The point to be made here is that a post hoc analysis of the system of community mental health reveals a covenant ontology.
One Unifying Truth of God as a World ViewCollins (1977) has approached the thesis of a covenant ontology as embodied through special revelation and general revelation. Special revelation refers to the explicit proclamation of the kerygma, the revealed Word of God, the Logos (John 1:1,2,14). Collins explains that the proclamation is revealed through "the Bible, a book that Christians believe to be God's written word of special revelation to man" (pp. 121122). In terms of general revelation, Collins describes it as the following:
General revelation, sometimes called natural revelation, refers to the truths that God has revealed himself through nature, science, or history; and which man can know by observation, empirical investigation, logical deduction, intuition, feeling, the study of tradition, or any other technique apart from reading the Bible. (p.121)
Upholding special revelation and general revelation is an ontological presupposition similar to Ogden's world view of covenant ontology. Collins describes his premise in terms of its implication for psychotherapy:
Let us consider the suggestion that, in the future, psychology could be more productive and less in a dilemma if it were built on the major premise that God exists and is the source of all truth. This assumption could serve as a starting point from which data could be collected, systems could be built, therapy could be developed, and principles of living could be derived. (p. 118)
There is only one source of truth and that is God's truth, This theme is central to Christian theology (Holmes, 1977). This same truth speaks to theology as well as community mental health. We see God's truth within the community mental health framework in the form of general revelation ("implicitly" in Oden's rubric).
The affirmation of community mental health by theology is rooted in the assumption of God as the source of all truth. Theology endorses community mental health in that special revelation (i.e. the Word of God) can describe and set the parameters within which general revelation may operate. For example, in describing the commandment of love, and specifically the description of love as being kind (I Corinthians 13:4), Smedes (1978) has stated that love is a "readiness to enhance the life of another person ... It is the power to move close to another person in order to heal" (p. 15). It means that love would not incarcerate a victim of mental distress to custodial care but would rather work toward the resolving of the person's distress through a community of care. The ontology of God's truth does not allow for the inhumane treatment of people. Theology is for that type of treatment that upholds the humanity of man as is the case in the field of community mental health.
If there is a covenant ontology, that all truth comes from God, then theology, by the act of affirmation justifies community mental health. However, in what way does theology affirm community mental health?
The Basic Underlying Assumptions of Community Mental HealthMann (1978) proposes a "mental health model" of community psychology that is rooted in the community mental health center movement. The purpose of this model is "to address the question of the impact of mental health services on mental health problems" (p.79). The nature of this type of service delivery is thought to have three basic assumptions: (1) emphasis on prevention, (2) focus on the concept of positive mental health, and (3) the social-environmental context as a highly influential source in the etiology of mental disorder. Theology speaks to all three assumptions.
Prevention and Positive Mental HealthThe concept of Positive mental health has grown out of the dissatisfactions with the medical model. This model purports that abnormal individual behavior can be attributed to some underlying cause or disease. The focus is on an intrinsic deficit or disorder which leads to interventions that involve treatment of a sick person to remove or alter the pathology that resides within the individual. Szasz (1974) clearly articulates the argument that there is no such entity as mental illness, rather, it is a myth. Mann states that a new definition of mental health is needed in order for efforts in prevention to move forward. He says that the outmoded definition of mental health as "the absense of mental illness" is both tautological and unproductive (1978, p.84).
|
Figure 1. An illustration of Lauden's model with the research traditions and theories defined. |
Theology affirms the importance of the social-environmental influences through the dynamic of Christian fellowship. It is essential for individuals to know they belong to a community and have a purpose in it.
Stir up the gift of God, which is in thee ... For God hath not given us the spirit of fear, but of power, and of love, and of a sound mind. (11 Timothy 1:6-7)
God has called His people to gather their resources to a life of courage and not of despair ... to utilize their God-given potentials not in timidity, but in power and in love. Indeed there is an inestimable worth in each person. This led the Psalmist to write astoundingly:
When I consider your heavens, the work of your fingers, the moon and the stars, which you have set in place, what is man that you are mindful of him, the son of man that you care for him? You made him a little lower than the heavenly beings and crowned him with glory and honor. (Psalms 8:3-5)
The question of "what is man?" has been a difficult one to answer both theologically and psychologically. The question is also central to the present discussion in that in the imago Dei some direction may be found as to theology's affirmation of positive mental health.
The Genesis account makes explicit the imago Dei: "So God created man in his own image, in the image of God he created him" (Genesis 1:27). Only human beings are made in God's image. They are distinct from the rest of living creation in that they alone may have a relationship with the Divine Being. Carey (1977) has stated that the stress of this passage is not on physical likeness, but that human beings transcend the earth by belonging to God. Thus, they must have a great deal of worth to be created by God and belong to Him. The imago Dei suggests that a human person is in a warm and intimate relationship with God. Thus, we see human beings as competent and valuable ... descriptions that are indicative of a positive, optimistic view for mental health.
Theology affirms the concept of positive mental health for reasons that persons were created in God's image ... an image that has an inalienable worth. The task that is inherent within the community mental health framework is to support, nurture, and build upon those areas within the individual that manifest God's image. Here again, the emphasis upon the strengths and potentials of the individual is paramount to a concept of positive mental health.
This part of the discussion on positive mental health is incomplete without mention of the Incarnation, for it is in Jesus Christ that we see who we are meant to be. The impact of his ministry on the history of mankind was that "he aroused men to realize their human predicament, and in his life he attracted men to a fulfillment of their humanity" (Carey, 1977, p.67). We see that human beings have a fallen nature, that they are alienated from God (Mark 2:8). Despite this fallen nature, Jesus reveals in his life what human beings are meant to be (Hebrews 4:15).
Mental illness is a complex problem with numerous determining factors. To reduce the etiology of mental illness to the human fallen nature overlooks a vast amount of insight and behavior that might enlighten any attempts at intervention. Community mental health opts for interventions that build upon the individual's potentials (those potentials being grounded in the imago Dei). Jahoda (1958) characterizes positive mental health as autonomy, integration, growth and self -actualization, positive attitudes toward the self, perception of reality, and environmental mastery. Phillips (1967) states that the development of competence or coping skills are also necessary for the concept of positive mental health. This same thought is in the Apostle Paul's writings:
By moving toward a positive approach in mental health, (especially in prevention) and out of the medical model, more of the human potential may be realized, or at least elicited, that individuals may, in the words of Soren Kierkegaard, "be that self which one truly is" (1941, p.29).Not that I have obtained all this ... but I press on to take hold of that for which Christ Jesus took hold of me. Brothers, I do not consider myself yet to have taken hold of it. But one thing I do: Forgetting what is behind and straining toward what is ahead, I press on toward the goal to win the prize for which God has called me heavenward in Christ Jesus. (Philippians 3:12-14)
Social and Environmental Context
Community mental health utilizes methods of intervention
within social systems. Moving away from the medical model
entails identifying the sources of mental disorder within the
immediate environment that surrounds an individual and
intervening in those social systems.
The impact of one's social-environmental context is highly nfluential upon one's mental health. Social support networks
affect individuals when they are recognized or defined as ill
and whether they can cope with stresses of community life
(Kaplan, 1977). Tolsdorf (1976) suggests that successful social
and community adjustment depends much upon the support
given to an individual by family and friends. By observing
beyond the individual in distress, a more comprehensive
approach to the alleviation of mental disorder can be made
possible.
Theology upholds this third assumption of community psychology. We see from Jesus' ministry that he was not restricted simply to minister to the needs of people in the synagogue nor did he passively wait for people to come to his dwelling place for healing. Instead, Jesus went into the community to provide healing to many sick people. In Mark 1:21-34 we find Jesus healing people in three contexts: in the synagogue, in the home of Simon and Andrew, and in the streets. In Matthew 4:23-24 Jesus went throughout Galilee teaching, preaching and healing. When the disciples were sent into the mission field Jesus gave them these instructions: "Do not go among the Gentiles or enter any town of the Samaritans. Go rather to the lost sheep of Israel" (Matthew 10:5-6). They were not to sit and wait for the lost sheep to find their way home.
One of the major distinctions of mental health workers of the community mental health variety is that they work in the community. They become both participants and observers of the community in which they work. The mental health worker must avoid retreating into the safety of the clinical office when it is evident that action within the community is preponderant. Taking Jesus' ministry as a model we see that community mental health serves as an example of how his ministry can be applied to the amelioration of mental distress.
Another major contention of the assumption of the social-environmental influence is that the individual cannot be viewed alone but must be seen in relation to the surrounding environment. The degree to which a person is isolated is a function of the person's relationship to the community, and hence, is central to an individual's wholeness. By isolating the person away from the community, the person loses a sense of wholeness. Klein (1968) reflects this idea:
They suffer from the agonizing anonymity of the perpetual stranger. Or they are oppressed by the sense of worthlessness and futility arising from the inability to influence the course of events. (p. 161)
Theology affirms the importance of the social-environmental influences through the dynamic of Christian fellowship (I Corinthians 12:12). It is essential for individuals to know they belong to a community and have a purpose in it. Each person (believer or non-believer) is given a gift that can be fulfilled within the community (I Corinthians 12:7). It is the natural endowment for the individual to belong to the community not only because the person has a contribution to make, but that it is part of God's design for creation: "But in fact God has arranged the parts in the body, everyone of them, just as he wanted them to be" (I Corinthians 12:8).. There is some inherent good in the existence of a unified community: "How good and pleasant it is when brothers live together in unity" (Psalm 133:1). Thus far community in this context means the fellowship of believers. However, to affirm the community importance in the secular realm, a model of Christian fellowship will provide a basis from which community mental health may borrow. The opinion of this author is that community mental health is already moving in the direction of embodying principles of Christian fellowship by exhorting the importance of community to the individual in distress.
In his book, Life Together, Bonhoeffer (1954) describes various ministries within the Christian fellowship. He notes a basic premise that is essential for an understanding of the community dynamic:
In a Christian community everything depends upon whether each individual is an indispensable link in a chain. . . It will be well, therefore, if every member receives a definite task to perform for the community, that he may know in hour of doubt that be, too, is not useless and unusable. (p. 94)
The community is an interdependent system. it means also
that the care of its individual members is vitally important.
The ministry of helpfulness (pp. 99-100) has its implica.
tions for the delivery of mental health services. Bonhoeffer
describes this as being available to God's will for doing His
service. Christians are not to filter out those tasks that may seem unattractive. This is juxtaposed with the need to deliver
services to the poor as well as to members of the often
neglected minority groups (Sue, 1977). Out of this ministry of
Jay M. Uomoto is a graduate of the University of Washington where he obtained a Bachelor of Science degree in Psychology. He is currently a doctoral candidate in clinical psychology at Fuller Theological Seminary, Graduate School of Psychology, where he also received a Master's of Arts degree in Theology. His research interests are in the areas of Asian American mental health, social support networks of chronic schizophrenics, and the application of learned helplessness theory to ethnic minorities. Clinical interests include cognitivebehavioral, brief, and family therapy techniques along with psychological assessment and behavioral medicine.
Two are better than one, because they have a good return for their work: If one falls down, his friend can help him up. But pity the man who falls and has no one to help him up! (Ecclesiastes 4:9-10)
The social-environmental influences also have an impact on
the mental health worker. This individual can also be aided
by the bearing of the burden by a significant other. This
principle has its counterpart in community mental health
through Gerald Caplan's
(1964)
system of mental health
consultation ... in particular the "counsultee-centered case
consultation." Here, the consultee is given advice and support
concerning a particular problem by another professional. The
mental health worker, too, is a part of the community, is
subject to the stresses of life and may at times need timely
support, care, and advice. Here is an example of the interdependency among the members in the community; each
member represents a part of the larger social system. Indeed,
the Christian model of ministry of bearing affirms those
principles and techniques in community mental health which
reflect that ministry.
The basic presuppositions of the community mental health orientation have been considered in light of theological perspectives. Now we must ask: Does theology affirm some changes that community mental health subscribes to that are considered to touch on some key issues in psychology today?
Nonprofessionals and ParaprofessionalsOne of the major shifts in the community mental health field has been in the area of mental health service delivery, more specifically, the shift from the professional agent to the nonprofessional and the paraprofessional. This has been born out of the serious gap between manpower resources and public needs. Iscoe (1971) suggests that an increase in manpower is essential to increase the effectiveness of the therapeutic agency. This increase in manpower focuses upon the non-professional in particular, not on the professional only, and it touches at the very core of psychology in that effective psychotherapy can be done by a non-professional as well as the professional. Theology affirms this notion.
A strong attack on professional elitism in the therapeutic agency has been made by Oden (1974), His claim is that
Professional elitism, whether in the clergy or in therapeutic circles, tends to assume that ordinary people cannot be therapeutic agents. (p. 9)
Research supports Oden's stance. Studies have shown that people turn to natural caregivers (who are also more available during a crisis) more often than to professionals in times of stress and emotional troubles (e.g. Lieberman, 1969). In a classic study by Bloch et al. (1963), it was found that lay training of specially selected persons could be as effective as those trained in a regular graduate school. The lay mental health counselor has also been found to facilitate significant improvement on hospitalized patient behavior (Carkhuff and Iruax, 1965). What seems to be central to any effective therapy, regardless of orientation, is what has come to be known as the "therapeutic triad": congruence, empathy, and unconditional positive regard (Rogers, 1957). These three characteristics need not be confined to or possessed solely by professionals.
The biblical account strongly supports the furthering and equipping of the laity. Jesus and his disciples were nonprofessionals (Acts 4:13) except for Luke, who was a doctor. Much of the early Christian witness was done through the ministry of the laity (Acts 8:1,4; 11:19-21). Jesus trained his disciples through instruction, modeling and by experience (e.g. Matthew 5:1-2; Luke 24:27; Acts 1:2). Though Jesus chose ordinary people to further his kingdom, he trained them carefully, nurturing them to the point that they could go out on their own into the mission field. Parallel to this in the field of community mental health, the training of lay therapeutic resources has taken place for the task of bridging the gap between the supply and demand of mental health services. Theology affirms those aspects of community mental health that support the use of the laity as therapeutic resources.
Therapeutic ConsiderationsOne of the primary antecedents to the onset of the community mental health movement was the dissatisfaction with psychotherapy. Eysenck's (1952) often cited criticism that psychotherapy is no more effective than the passage of time and placebos stands as one of the classical statements against psychotherapy. Other research however, suggests a more positive outcome for the effectiveness of therapy (Bergin, 1963). The implication of unsuccessful psychotherapy has led workers in the community mental health field to move on to different roles (e.g. community psychologists, social action psychologists, social engineers, as suggested by Scribner, 1968). Must traditional psychotherapy be abandoned? The Christian doctrine of man may shed light upon the preserva tion of the traditional psychotherapeutic agency, however with certain ramifications.
Schmieding (1958) has stated that "man is not now a soul then again a body. Man is a single being, a self, an I, or a you" (p. 318). The implication is that man is a single entity; man is whole ... not in duality (body and soul) or trichotomy (body, soul, and spirit). Berkouwer (1962) has said that "we should remember that it is the whole man who is restored and saved" (p. 229). Therefore, when viewing through the psychotherapeutic agency, we see man as unity and as whole.
Because man is whole, a unity, an equally complementary treatment must be aimed toward the whole man. This is not to say that psychology must formulate a new quasitherapeutic orientation as a means of therapy. Rather, an eclectic approach to community mental health may be more useful in the light of God's truth, An examination of the biblical text finds Jesus using a variety of techniques. The doctrine of the whole man, and Jesus'example of the number of ways he dealt with the whole man, is evidence for an eclectic approach to therapy (e.g. Garfield, 1980) and service delivery. This eclectic approach has become a reality within the community mental health center in terms of the types of services available. They are: inpatient care, outpatient care, emergency services, partial hospitalization, consultation, education, diagnostic services, training, and research and evaluation. The comprehensive approach to mental health in the community mental health center does reflect the need to minister to the whole man.
The inequality of treatment rendered to individuals in distress has become an increasingly important issue. Clients receive differential treatment in therapy depending upon demographic factors such- as age, race, sex, and socioeconomic factors (Overall and Aronson, 1962). The YAVIS Syndrome has been suggested by Schofield (1964) as a characterization of the desirable client. He found that therapists prefer Young, Attractive, Verbal, Intelligent, and Successful individuals for clients. Goldstein and Simonson (1971) suggest that there is a greater need for research and intervention that is focused on the HOUND patient: the Homely, old, Unattractive, Nonverbal, and Dumb client. It seems as if a person's natural endowment determines the type of care that person receives. Jesus addressed this issue:
For I was hungry and you gave me something to eat, I was thirsty and you gave me something to drink, I was a stranger, and you invited me in ... I tell you the truth, whatever you did for one of the least of these brothers of mine, you did for me. (Matthew 25:35-40)
Jesus cared for the sick, the lepers and the blind. Jesus ministry is a model for human response. Humankind's response to human need is, in actuality, a response to the Divine Being Himself. Community mental health is in a sense a human response to the needs of the individual by going into the community, meeting distressed people where they are ... not in a selective manner as is characterized by the private practice model.
The inequality of treatment is overtly exemplified by the treatment rendered to members of different minority groups. Research has shown that minority clients are discharged more quickly (from inpatient services) and are more often seen for minimal supportive psychotherapy rather than individual or group therapy (Sue, 1977).
When Jesus said "come to me, all you who are weary and burdened, and I will give you rest," he did not mean to exclude any person. Jeeves (1976) affirms this point by saying that because man was made in the image of God, that fact alone "spelt out the equality of all men before God, so within the community of the new humanity there can be no division of race or class (p. 75). "
Community mental health is slowly taking up the task of
rendering services to minority group members with the
utilization of bilingual therapists and services that are placed
within particular ethnic communities. Theology affirms those
aspects of community mental health that upholds God's
design for the essential equality among humankind.
Conclusion
Community mental health has been shown to be affirmed by and integrated with theology through the concepts of prevention, positive mental health, and social-environmental influences. Each of these have roots in a common world view which is taken from Oden's rubric of "covenant ontology" and Collins' premise of God's truth being the source of all truth. From this world view a topical consideration of various methods, dynamics, and services within the community mental health orientation reveals that theology affirms each area.
It is the hope of this author that mental health workers, as well as the community at large, may become uniquely involved in community mental health, a field that embodies much of God's truth. May they contribute and further draw attention to the agapic type of love that is so inherently necessary to the healing and growth of individuals. Karl Barth (1958) wrote about the kind of love that may form a foundation to the discipline of community mental health:
Christian love turns to the other purely for the sake of the other. It does not desire it for itself. It loves it simply because it is there as this other, with all its value or lack of value. It loves it freely. (p. 733)
Indeed ' agapic, love needs to be at the foundation of such a system. To this, theology may be more than just for Community mental health.
REFERENCESBergin, A.E. The effects of psychotherapy: Negative results revisited. Journal of Counseling Psychology, 1963, 10, 244.
Berkouwer, G.C. Man: The image of God. Grand Rapids, Michigan: Eerdmans, 1962.
Bonhoeffer, D. Life together. New York: Harper & Row, 1954.Caplan, G. Principles of preventative psychiatry. New York: Basic Books, 1964.
Carey, G. I believe in man. Grand Rapids, Michigan: Eerdmans, 1977.Carkbuff, R.R. & Truax, C.B. Lay mental health counseling: The effects of lay group counseling. Journal of Consulting Psychology, 1965,29, 426-431.
Collins, G.R. The rebuilding of psychology: An integration of psychology and Christianity. Wheaton, Illinois: Tyndale, 1977.
Dunham, H.W. Community psychiatry: The newest therapeutic bandwagon. Archives of General Psychiatry, 1965, 12, 303-313.
Eysenck, H.J. The effects of psychotherapy: An evaluation. Journal of Consulting Psychology, 1957, 21, 95-103.
Garfield, S.L. Psychotherapy: An eclectic approach. New York: Wiley, 1980.Goldstein, A.D., & Simonson, N. Social psychological approaches to psychotherapy research. in A. Bergin & S. Garfield (Eds.). Handbook of psycho therapy and behavior change. New York: Wiley, 1971.
Hobbs, N. Mental health's third revolution. American Journal of Orthopsychiatry, 1964,34,1-20.
Holmes, A. All truth is God's truth. Grand Rapids, Michigan: Eerdmans, 1977,
Iscoe, 1. Professional and subprofessional training in community mental health as an aspect of community psychology. In Task Force on Community Mental Health, Division 27 of the American Psychological Association. Issues in community psychology and preventative mental health. New York: Behavioral Publications, 1971.
Iscoe, I., & Spielberger, C. The emerging field of community psychology. In 1. Iscoe & C. Spielberger (Eds.). Community psychology: perspectives in training and research. New York: Appleton-Century-Crofts, 1970.
Jahoda, M. Current concepts of positive mental health. New York: Basic Books, 1958.
Jeeves, M.A. Psychology and Christianity: The view both ways. Downers Grove, Illinois: Intervarsity Press, 1976.
Kaplan, B.H., Cassel, J.C., & Gove, J. Social support and health. Medical Care, 1977,15,47-50.
Kierkegaard, S. The sickness unto death. Princeton University Press, 1941.Klein, D.C. Community dynamics and mental health. New York: Wiley, 1968.
Korchin, S.J. Modern clinical psychology. New York: Basic Books, 1976.Laudan, L. Progress and its problems. Berkeley: University of California Press, 197T
Lieberman, R. Police as a community mental health resource. Community Mental Health journal, 1969, 5, 111-120.
Mann, P.A. Community psychology: Concepts and applications. New York: The Free Press, 1978.
Oden, T.C. After therapy, what? N. Warren (Ed.). Springfield, Illinois: Thomas, 1974.
Oden, T,C. Kerygma and counseling: Towardacovenant ontology for secular psychotherapy. New York: Harper & Row, 1978.
Overall, B., & Aronson, A. Expectations of psychotherapy in lower socioeconomic patients. American Journal of orthopsychiatry, 1962, 32, 271-27Z
Phillips, L. The competence criterion for mental health programs. Community Mental Health journal, 1967, 3, 73-76.
Rioch, M.J., Elkes, C., Flint, A.A., Usdansky, B.S., Newman, R.G., & Silber, F_ National Institute of Mental Health pilot study in training mental health counselors. American Journal of Orthopsychiatry, 1963, 33, 678-689.
Rogers, C. The necessary and sufficient conditions of therapeutic personalih. change. Journal of Consulting Psychology, 1957, 21, 95-103.
Sarbin, T.R., & Mancuso, J.C. Failure of a moral enterprise: Attitudes of the public toward mental illness. Journal of Consulting and Clinical Psychology,1970,35,159-173.
Schmieding, A.F. The dualism problem. In P.E. Meehl (Ed.). What, then, man? St. Louis: Concordia, 1958.
Schofield, W. Psychotherapy: The purchase of friendship. Englewood Cliffs, New Jersey: Prentice-Hall, 1964.
Schribner, S. What is community psychology made of? Division of Community Psychology, Newsletter, 1968,2, 4-6.
Smedes, L.B. Love within limits . Grand Rapids, Michigan: Eerdmans, 1978.Sue, S. Community mental health services to minority groups: Some optimism, some pessimism. American Psychologist, 1977,32,616-624.
Szasz, T.S. The myth of mental illness: Foundations of a theory of personal conduct. New York: Harper & Row, 1974.
Tolsdorf, C. Social networks, support and coping. An exploratory study. Family Process, 1976, 4, 407-418.